All text below has been revised and condensed, please view original text at Aaron Swanson.
Separating foot types into supinators or pronators may provide adequate assessment for treatment. However, for a more specific treatment plan it would be advantageous to understand the possible abnormalities and pathomechanics of the forefoot and rearfoot (calcaneus). More importantly, knowledge of these abnomalities/pathomechanics will also prevent deleterious treatment.
For example, providing medial calcaneal mobilizations/releases for the overpronator would be great if the patient has a compensated calcaneal varus. But if the patient has a compensated forefoot varus the medial mobilization/release would likely worsen their injury. It may sound complicated, but once you understand these 3 foot abnormalities and pathomechanics it will make sense.
Foot Pathomechanics = compensations that occur from foot abnormalities during weight bearing tasks
The 3 Foot Abnormalities
- Calcaneal (Rearfoot) Varus
- Forefoot Varus
- Forefoot Valgus
Basic Foot Knowledge
The foot can be simplified into a structure that has 2 jobs: mobility (pronation) and stability (supination). It requires adequate mobility to adapt to ground surfaces and facilitate shock-absorption. It requires stability to function as a rigid lever for efficient propulsion. Failure of either of these jobs will cause great dysfunction throughout the body.
This stability and mobiilty is dependent on an intricate passive and dynamic system. The passive system of bone orientation and joint congruency help to provide static stability when aligned, and flexibility when not aligned. The dynamic system of the muscles help to reinforce stability and allow for controlled flexibility (eccentric loading). When there is an abnormality in the foot alignment or structural, the subtalar joint often compensates by altering the normal balance of stability and mobility.
Treating the compensation may provide the patient relief. But for full resolution of the dysfunction you will need to correct and remove the cause.
Normal Foot
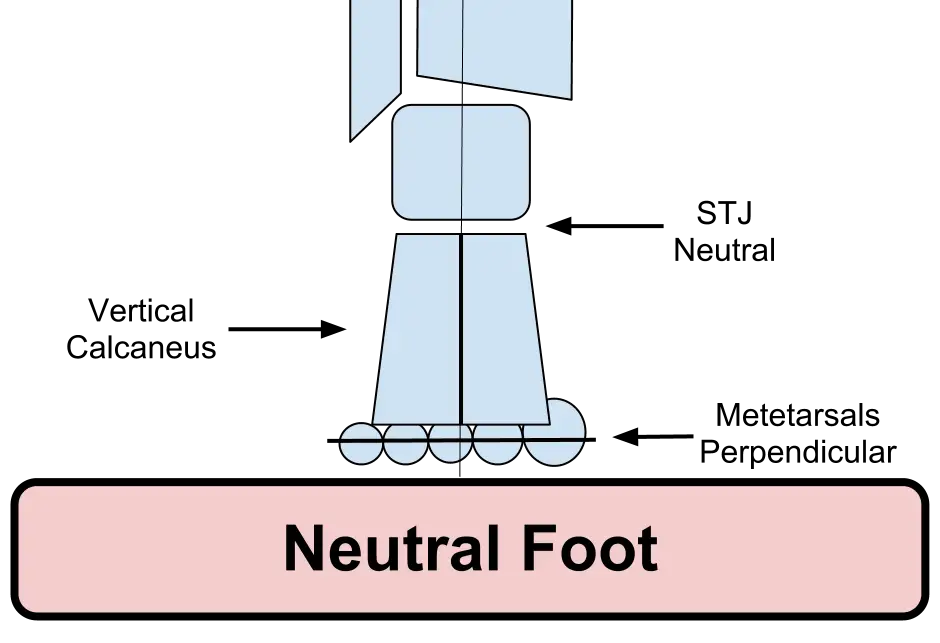
Normal neutral foot alignement is compromised of 3 things:
1) Neutral Subtalar Joint
2) Vertical Calcaneus (in line with lower leg)
3) Metatarsal Heads Perpendicular to neutral calcaneus/subtalor joint.
…This is the position for optimal functioning of both passive and dynamic systems.
Assessment
Postural assessments should be viewed from all angles.
- Anterior view for frontal plane deviation (forefoot abduction).
- Oblique view for a good assessment of the arch and navicular height.
- Posterior view to display calcaneal and subtalar positions.
Once you have a postural assessment, it is important to determine the foot alignment and structure. There are many ways to accomplish this:
- Finding talar neutral (anterior palpation in supine)
- Lower leg to rearfoot alignment
- Unbiased passive dorsiflexion
- Joint play
- Postural foot assessment (standing)
- Gait analysis.
I find it best to use a combination of these assessments. If you understand the possible types of pathomechanics and forefoot/rearfoot alignment it will make it easier to determine exactly which foot type your patient has.
Finally, you want to analyze their gait to see how the patient dynamically uses their foot alignment and structure. The static postural foot assessment will help give you an indication of what you should be looking for during the analysis. You want to not only look for over or under pronation, but try to assess for 3 specific aspects of the dysfunctional motion (compensation). This is of paramount importance because it is the compensations that will dictate which structures you need to treat.
3 Aspects of Dysfunctional Motion
- Amount/range of Motion
- Speed of the Motion
- Timing of the Motion
Calcaneal Varus
This is the most common foot abnormality. However, it may or may not be a clinical problem.
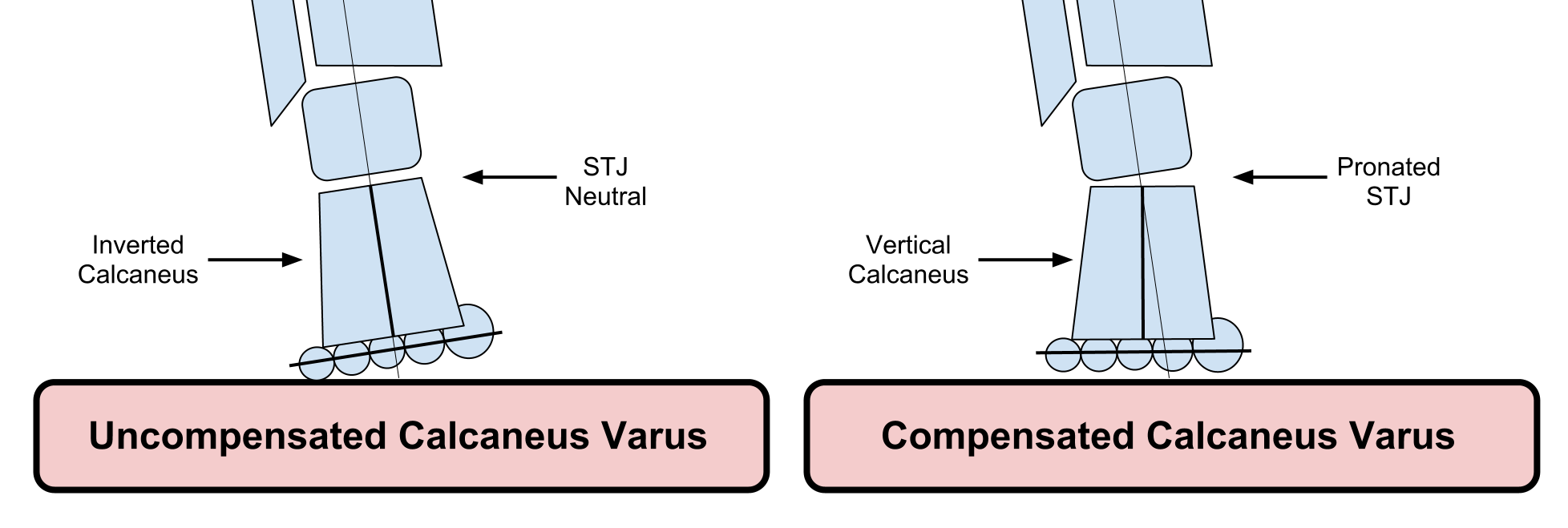
Calcaneal varus is when the calcaneas is inverted with the subtalar joint in neutral (full contact) and the forefoot is perpendicular to the lower leg. This foot abnormality is more supinated at heel strike. These patients often present with decreased lateral (eversion) subtalor joint play.
Compensations include:
- Overpronation (mid foot allows calcaneus to sit flush on floor)
- 1st ray plantarflexion for ground contact (calcaneal pressures are more lateral due to its inversion remaining).
Posture Assessment
Uncompensated (referring to the calcaneus)
= Calcaneus Inverted & Navicular Raised (Supinated)
Leading to: Plantarflex 1st Ray (distal) & Tibial Varum (proximal)
Compensated (referring to the calcaneus)
= Calcaneus Vertical & Navicular Collapse (Pronated)
Gait Assessment
Abnormal compensatory pronation (amount & speed) will occur at heel strike and continue until heel rise. After the heel is off the ground the foot is able to supinate in time for a fairly normal propulsion. These patients differ from forefoot varus in that the calcaneus does not go into excessive valgus (eversion).
Forefoot Varus
This is the most destructive foot abnormality to the lower extremity. Because of this, it is the most clinically common pathomechanical abnormality.
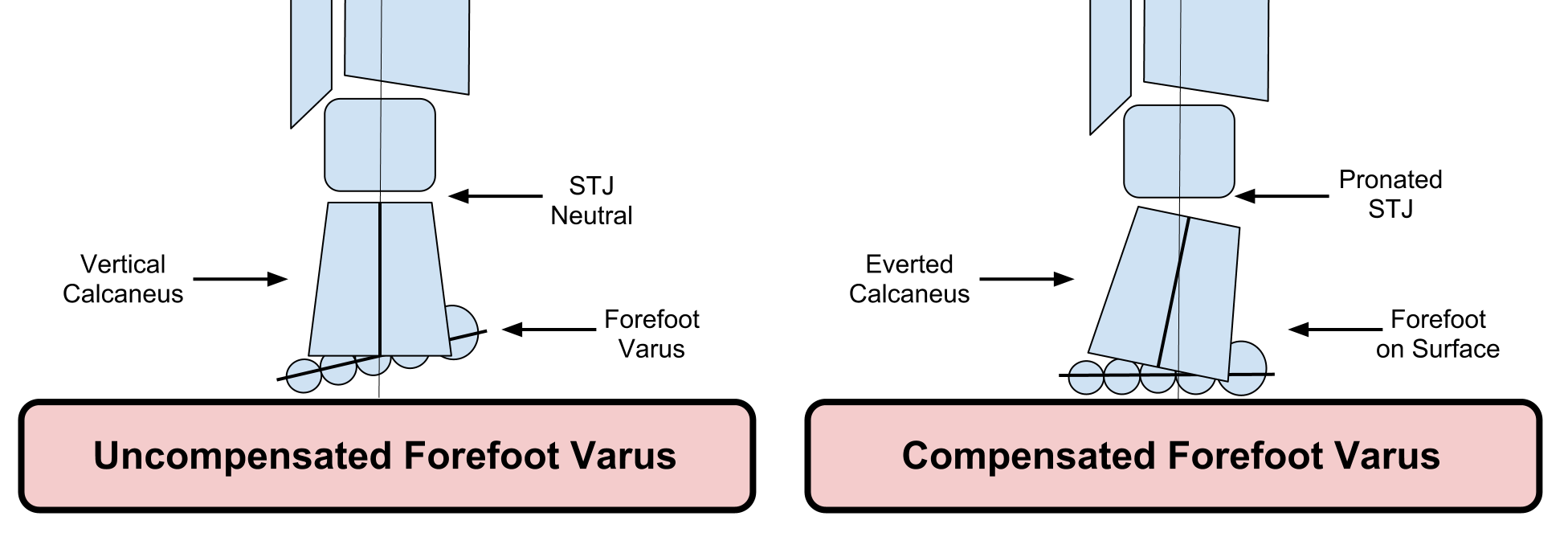
Forefoot varus is when the forefoot is inverted (big toe higher than 5th toe) while the subtalar joint and calcaneus are in neutral. This foot abnormality almost always causes over pronation. Joint play is often excessive.
Compensations include calcaneal eversion and navicular collapse to allow forefoot to contact the surface.
Posture Assessment
Uncompensated (very uncommon)
= Calcaneus Vertical & Navicular Raised
‘Supination’ posture, lateral foot weight shift, 1st ray off ground.
Compensated
Calcaneal Valgus (everted) & Navicular Collapse & Forefoot Abduction (to achieve MT1 ground purchase)= Pronated
Gait Assessment
To allow for the inverted forefoot to contact the ground there is excessive compensatory pronation (amount & timing) beginning at the foot flat phase of the gait cycle. This continues for the rest of the stance phase, causing the patient to push-off with an unlocked pronated foot. This is a major clinical problem since push-off requires a rigid supinated foot to use as a lever for propulsion. These patients differ from calcaneus varus because they are not able to achieve any supination prior to push-off.
Forefoot Valgus
This foot abnormality often presents in patients with rigid and supinated feet (unlike forefoot varus). Since they are already in a supinated posture they are at higher risk for inversion ankle sprains.
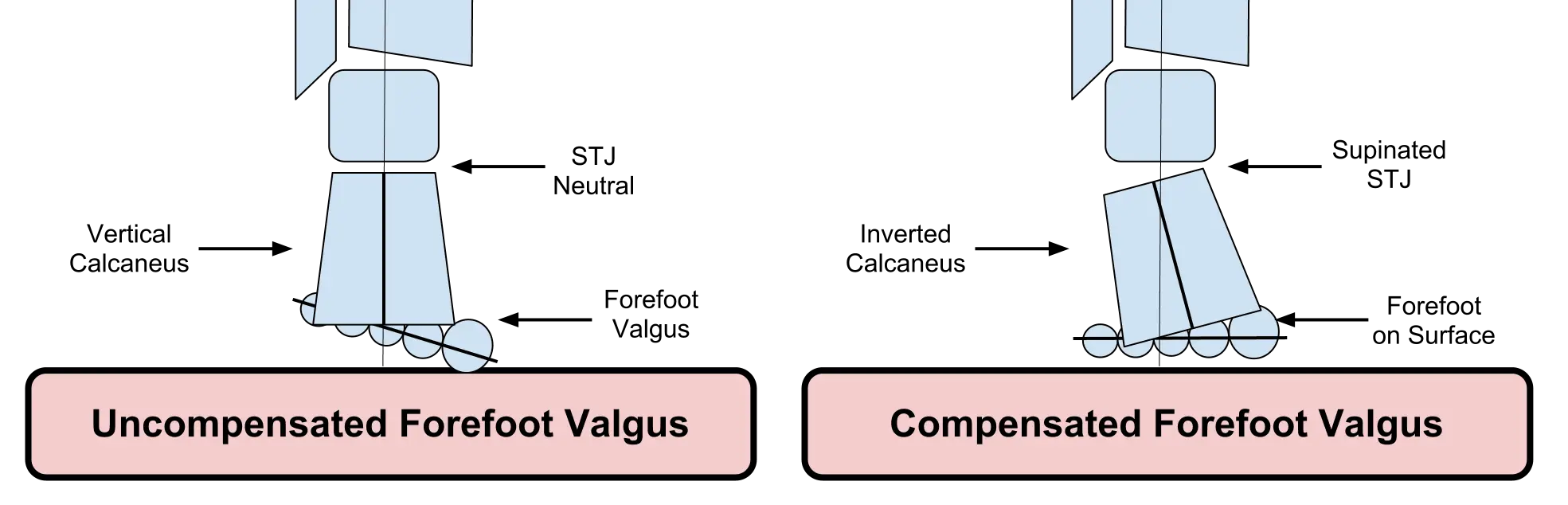
Forefoot valgus is when the forefoot is everted while the calcaneus and subtalor joint are in neutral. The medial metatarsals lie below the calcaneus (plantar flexed in relation to the calcaneus). There are two different types: total valgus (all the toes slope down) or 1st ray plantarflexion. This foot type often presents with restricted joint play (midfoot, 1st ray, calcaneus).
Since the metatarsals lie below the calcaneus it is nearly impossible not to compensate. The patient must supinate to accomodate this abnormality. This may lead to a calcaneal varus compensation.
Postural Assessment
Uncompensated
Very uncommon – would cause a significant amount of increased pressure on the first ray
Compensated
Calcaneal Varus (inverted) & Naviclar Raised = Supinated
Gait Assessment
Excessive compensatory supination occurs (amount & timing) after heel strike due to premature loading of the forefoot. Pronation is insufficient, but may occur at the end of stance phase to allow for knee flexion. This foot abnormality has trouble attenuating loading forces, thus proximal joints are forced to accomodate.
Bottom Line
It is important to note that these abnormalities and pathomechanics are not black and white. They exist on a continuum and are often times combined. Being able to further assess your pronators and supinators into a specific pathomechanical foot type will improve your plan of care and allow you to provide your patients with specific interventions to fix the culprit of the problem.
Supinators (Pes Cavus)
–> Uncompensated Calcaneal Varus & Compensated Forefoot Valgus
Pronators (Pes Planus)
–> Compensated Calcaneal Varus & Compensated Forefoot Varus
While this post focused specifically at the local foot and ankle joint, it’s important to consider regional interdependence. Remember that the height and rigidity of the arch can be affected by tibial internal and external rotation (in closed chain). And this tibial motion is further influenced by it’s proximal structures.
Dig Deeper
Somastruct – Forefoot Varus – Overpronation – Intrinsic Foot Strengthening – Arch Strengthening
Physioblogger – Plantarflexed 1st Ray
References
Tiberio D. Pathomechanics of Structural Foot Deformities. PHYS THER. 1988; 68:1840-1849. (A Must Read)
Donatelli R. Abnormal Biomechanics of the Foot and Ankle. J Orthop Sports Phys Ther 1987;9(1):11-16.
Brown LP, Yavorsky P. Locomotor biomechanics and pathomechanics: a review. JOSPT 1987;9(1):3-10
